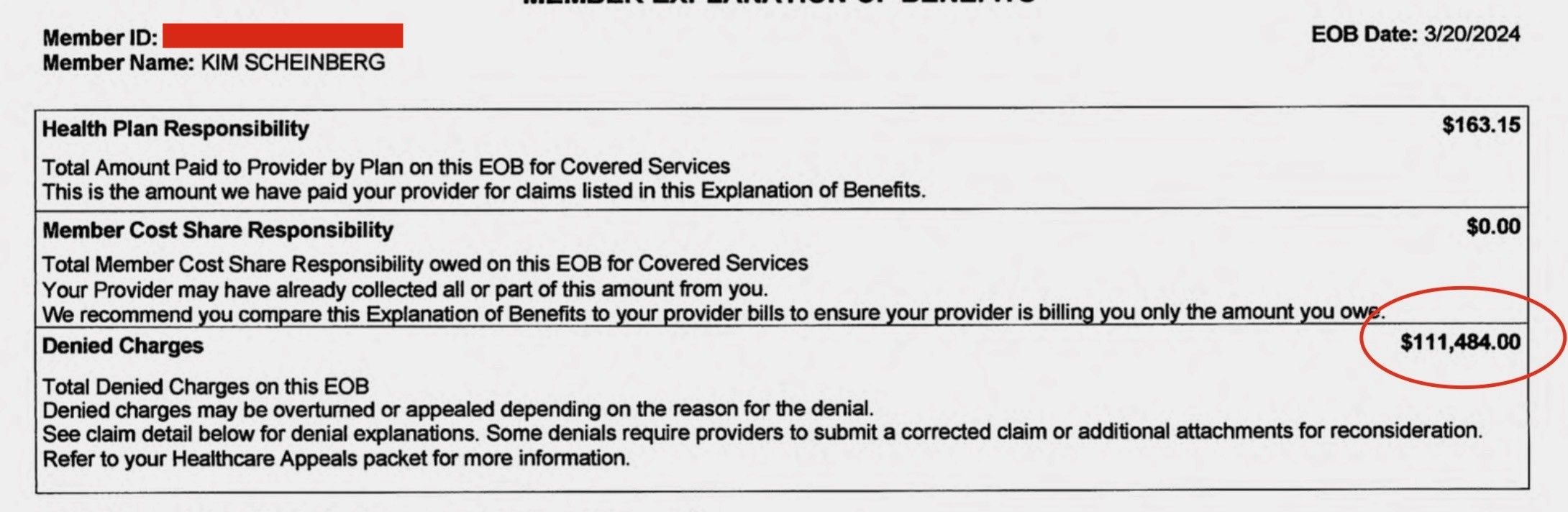
Date: 3/20/2024 Member Name: KIM SCHEINBERG Health Plan Responsibility $163.15 Total Amount Paid to Provider by Plan on this EOB for Covered Services This is the amount we have paid your provider for claims listed in this Explanation of Benefits. Member Cost Share Responsibility $0.00 Total Member Cost Share Responsibility owed on this EOB for Covered Services Your Provider may have already collected all or part of this amount from you. We recommend you compare this Explanation of Benefits to your provider bills to ensure your provider is billing you only the amount you owe Denied Charges $111,484.00 Total Denied Charges on this EOB Denied charges may be overturned or appealed depending on the reason for the denial. See claim detail below for denial explanations. Some denials require providers to submit a corrected claim or additional attachments for reconsideration. Refer to your Healthcare Appeals packet for more information.
{kind=link}
https://media.mas.to/media_attachments/files/113/891/984/840/701/232/original/facc2d5c46e98df8.jpeg